
Latest News

A blue SUV remains in a ditch after an early-morning crash along Segar Mountain Road in Kent May 27.
Ruth Epstein
The driver was transported to Danbury Hospital with minor injuries, according to police.
The damage to a utility pole forced crews to shut down parts of the road and reduce traffic to a single lane throughout the day. First Selectman Eric Epstein announced that traffic would be impacted as utility companies make repairs. Motorists were advised to avoid the area until the work is complete.
As of 2 p.m., traffic at the scene was reduced to alternating single lane travel. Employees from Eversource Energy, Aquarion Water Company and the state Department of Transportation were at the site making repairs to the utility pole and wiring. They have yet to provide an estimate for when the repairs will finish.
The car was still in the ditch as of mid-afternoon, officials on the scene said.
In an email to Kent residents, which was sent at approximately 12:40 p.m., Epstein reported that a water line connected to one residence in the area was also damaged, but clarified that it was not the line supplying the town.
 Repair crews respond to an early-morning crash along Segar Mountain Road in Kent that damaged a utility pole and water line. Ruth Epstein
Repair crews respond to an early-morning crash along Segar Mountain Road in Kent that damaged a utility pole and water line. Ruth Epstein



Want more of our stories on Google? Click here to make us a Preferred Source.
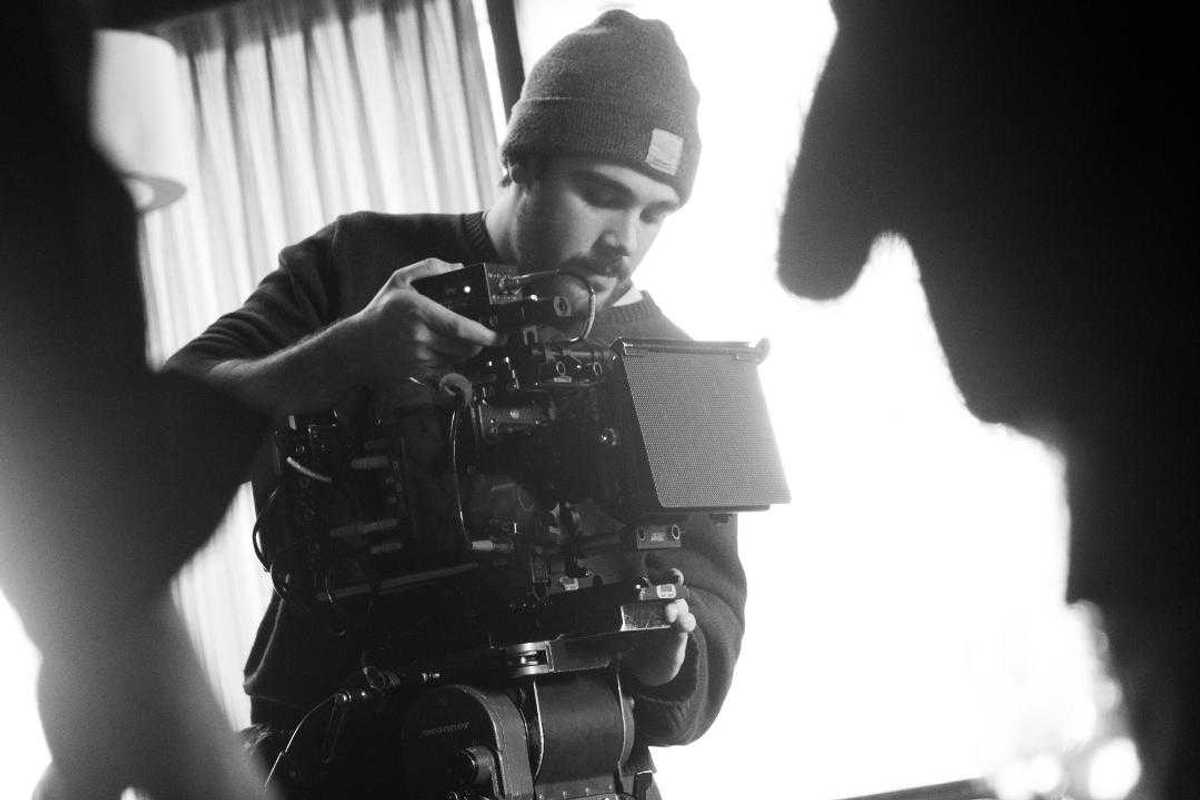
Filmmaker Yonah Sadeh on a shoot last year in New York City.
Matt Kashtan
It is an exciting opportunity for Sadeh, who has built his own business, Sadeh Studios, by working with small area businesses and nonprofits, “helping to tell their stories through film,” he said.
Some of his projects have included projects for local affordable housing organizations and area nonprofits such as Berkshire Busk, Berkshares, Naturalis Healing, local after-school programs and the Falls Village Fire Department. Current projects are for Berkshire Mountain Bakery and a documentary about Great Barrington’s revitalization in the 1990s.
Sadeh discovered early in life that he wanted to make films and began to develop his process and distinct style.
“It started with puppet shows and musical performances, and then, when I was around 12, a family friend showed me how to use my family’s computer to record and edit short homemade videos using iMovie. From that point on, it was pretty much all movies. I would set up my mom’s computer on a stack of books and record with the webcam.”
An early influence was Wes Anderson’s “Fantastic Mr. Fox,” which, “inspired my Claymation videos when I was 10 and remains one of my favorite films.”
He said getting his first camera made a big difference in his filmmaking.
“I was no longer stuck filming wherever I could set up the laptop. I could move with the camera and be more intentional about how things looked.”
Finding some of the technical aspects challenging, he watched YouTube to learn.
“I would imagine these big scenes, like fight sequences with lighting and effects, and then have to figure out how to actually make them. That process pushed me to learn. I spent a lot of time watching people like Casey Neistat, Film Riot and Corridor Digital, and just trying things out.”
Knowing the path he wanted to take, he pursued his high school education at Bard College at Simon’s Rock in Great Barrington, MA. The school has since relocated to Barrytown, New York.
“Simon’s Rock was not a film school in a traditional sense, but it had incredible faculty that I was able to work with one-on-one throughout my years there,” he said. “It gave me the flexibility and time to make films both in and outside of class, and to start my production business while still in school.”
He was able to take college-level film courses while still in high school.
“It seemed like the perfect opportunity. I loved it so much that I stayed at Simon’s Rock after graduating from the academy for my bachelor’s degree.”
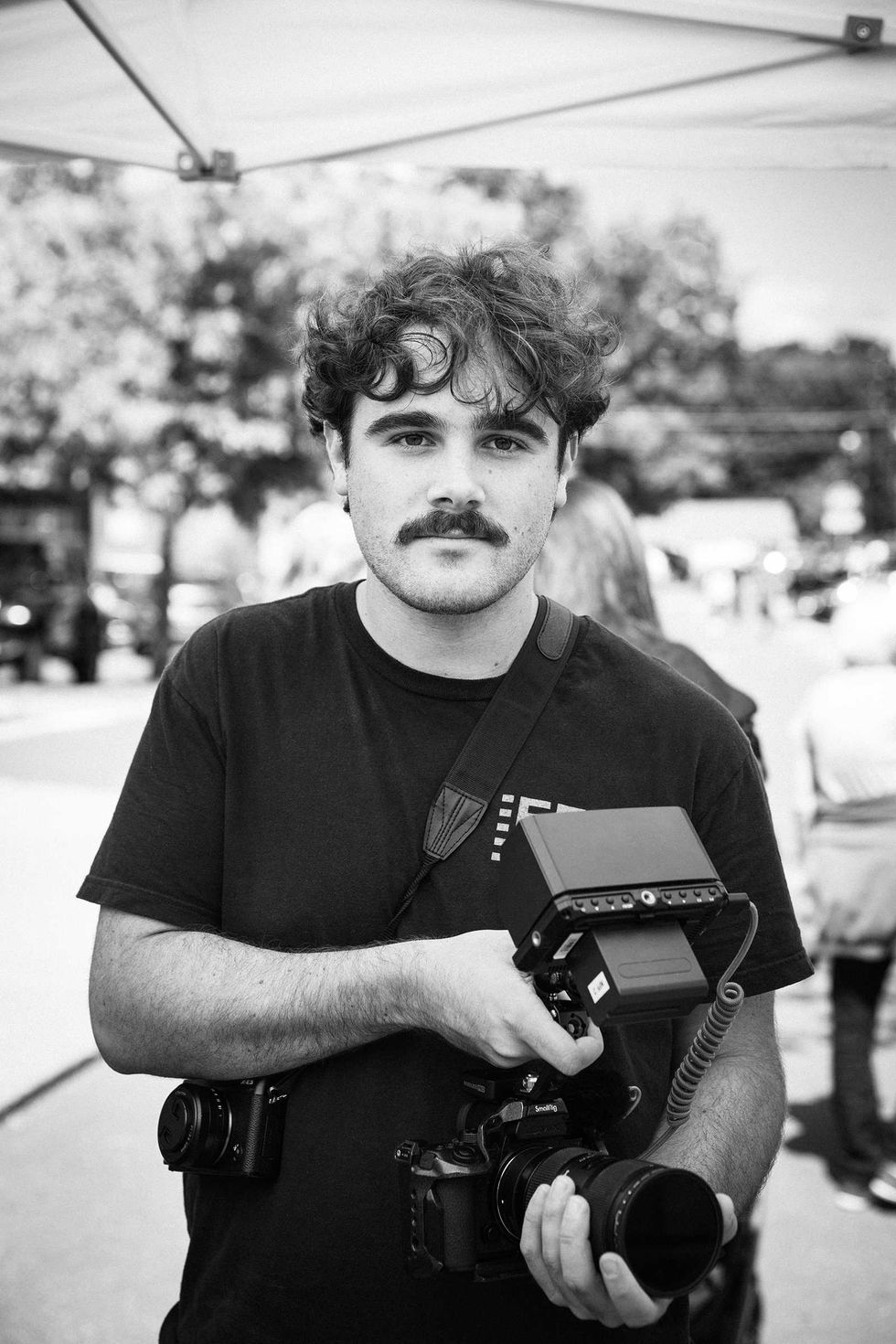 Filmmaker Yonah Sadeh at work. Lisa Volmer
Filmmaker Yonah Sadeh at work. Lisa Volmer
After graduating, he focused full time on his freelance business.
“Most of my professional work is in documentary, where I am a one-man crew overseeing every aspect of the process, from meeting with clients to develop the idea to planning, filming and editing it all together. I love working in this way, with my hands in every part of the project.”
In addition to documentaries, he also works on narrative films.
“The script I am working on now is set over the summer solstice and follows two kids over a short but formative period of time. I feel like this idea of land and place, and the passing of time, is a pretty consistent theme in all of my work, both narrative and documentary.”
Narrative films involve working with a crew, and he said writing and directing have presented different challenges.
“By the time I get to production, I’ve usually been sitting with the story for a while and have a pretty clear picture of how I want each scene to feel. So a lot of directing is about communicating that vision to the actors and crew. It can definitely be stressful, especially with the pressure of being on set. But I’ve been lucky to work with people I really trust and enjoy collaborating with, which makes a big difference.”
The finished film, Sadeh said, “becomes something built by everyone involved.”
Eager to share his love of filmmaking, Sadeh recently took on the role of curator of the VideoWall at the Hunt Library in Falls Village.
“I would love the VideoWall to become a place that showcases the work of local filmmakers, and I hope that other creatives in the area will submit their work to be shown.”
Reflecting on his chosen path, Sadeh said, “I feel really excited and creatively fulfilled to be doing the work I love in the place I grew up.”
Learn more at sadehstudios.com


Want more of our stories on Google? Click here to make us a Preferred Source.



